

Direct Answer: Whether a root canal is the right call depends on how much healthy tooth structure remains and whether the infection is still containable. If the tooth can be saved, root canal therapy is usually the most conservative path.
If you’ve been searching for an alternative to root canal, you’re not alone — and you’re probably not searching out of curiosity. More likely, you’ve got tooth pain that’s been building for a few days, you’ve heard root canals are brutal, and you’re hoping someone on the internet will tell you there’s an easier option. That anxiety is understandable. The reputation root canals carry is mostly decades out of date, but it sticks around.
The real question isn’t whether you can skip the procedure — it’s whether root canal therapy is actually the right treatment for your specific tooth. Sometimes it is. Sometimes it genuinely isn’t. The decision comes down to clinical factors your dentist can evaluate with an exam and X-rays, not a preference or a judgment call.
This article walks through how that decision actually gets made: what makes a tooth a candidate for root canal therapy, what situations point toward extraction and replacement instead, and why timing plays a bigger role than most patients realize.
What Root Canal Therapy Is Actually Trying to Do
Start with the anatomy. Every tooth has an outer shell of enamel and dentin, and inside that shell is a soft tissue called the pulp. The pulp contains nerves and blood vessels. When a tooth gets deeply decayed, cracked, or traumatized, bacteria can reach the pulp and cause an infection.
That infection is what produces the deep, throbbing pain patients describe — and left alone, it spreads. It can move from the pulp into the surrounding bone, forming an abscess that becomes much harder to treat.
Root canal therapy removes the infected or inflamed pulp tissue, cleans the inside of the tooth, and seals it off. The tooth stays in place. You keep the root, you keep the bone around it, and after a crown is placed on top, the tooth functions normally. The goal is to stop the infection while preserving what’s already there.
This matters because a natural tooth — even one that’s been through endodontic treatment — almost always performs better long-term than a replacement. It maintains the bone underneath it. It responds to bite pressure the way your other teeth do. And it doesn’t require the surrounding teeth to be modified, the way a bridge does.
For most patients with an infected tooth that still has adequate structure, root canal therapy is the most conservative path available. It’s not the aggressive option — extraction is.

When a Root Canal Is the Right Answer — and When It Isn’t
Root canal therapy works when the infection is contained to the pulp and the tooth structure around it is still solid enough to support a crown afterward. That combination — treatable infection, salvageable structure — is the scenario where endodontic treatment makes the most sense.
But there are situations where it genuinely isn’t the answer:
- The tooth is fractured below the gumline. A crack that extends beneath the bone level can’t be sealed effectively, and the tooth won’t hold a crown. Extraction becomes necessary.
- There isn’t enough tooth structure left. If decay has destroyed most of the crown portion of the tooth, there may not be enough material remaining to restore it after root canal therapy. You’d be doing the procedure and still losing the tooth.
- A previous root canal has failed and retreatment isn’t viable. Retreatment works in many cases, but if the infection has returned and the anatomy makes it impossible to fully clean and reseal, the calculus shifts toward extraction.
- The surrounding bone has been severely compromised. Advanced infection or periodontal disease can destroy the bone that supports the tooth’s root, leaving nothing stable to preserve.
In any of these scenarios, extraction followed by an implant or a bridge becomes the more realistic path. That’s not a failure — it’s the right clinical decision for that tooth at that stage.
If you’re weighing what comes after an extraction, When Is a Dental Implant the Right Choice After Tooth Loss? walks through how that decision gets made. And if you’re curious about timing, How Long Does the Dental Implant Process Actually Take? gives a realistic picture of the full timeline.
Root Canal vs. Extraction and Implant: A Side-by-Side Look
These aren’t competing options in every case — but when both are on the table, here’s how they compare across the factors patients usually ask about most.
| Factor | Root Canal + Crown | Extraction + Implant |
|---|---|---|
| Natural tooth preserved | Yes | No — tooth is replaced |
| Bone loss after treatment | Minimal — root maintains bone | Some bone loss without implant; implant slows it |
| Number of appointments | 2–3 typically | 3–5+ depending on bone grafting needs |
| Typical cost in South King County | $1,200–$2,200 combined (RCT + crown) | $3,000–$5,500+ for implant and crown |
| Recovery time | 1–3 days discomfort typical | Longer — implant integration takes 3–6 months |
| Long-term success rate | High when tooth structure is sound | High — implants have strong long-term track records |
| Best candidate | Infected pulp, intact structure | Tooth unsalvageable or already extracted |
Why Timing Changes What’s Possible
Form submissions and phone calls to practices like ours often describe the same pattern: molar pain that started a week or two ago, maybe longer, that the patient kept hoping would resolve on its own. It’s one of the most common ways people arrive at this decision.
The clinical reality is that an infected tooth doesn’t stay stable while you wait. Bacterial infection spreads. What starts in the pulp can move into the surrounding bone. A tooth that was a clean candidate for root canal therapy two weeks ago can reach a point where the structure is too compromised to save.
This isn’t meant to scare anyone into rushing — it’s just the honest picture of what changes over time. A tooth that can be saved with endodontic treatment today may require extraction six weeks from now, which means a longer process, more cost, and more recovery. Understanding that helps patients make an informed decision about when to get evaluated, not a fear-driven one.
If the pain has been building, even off and on, that’s worth having looked at sooner rather than later. An exam and X-rays will tell you exactly where things stand.
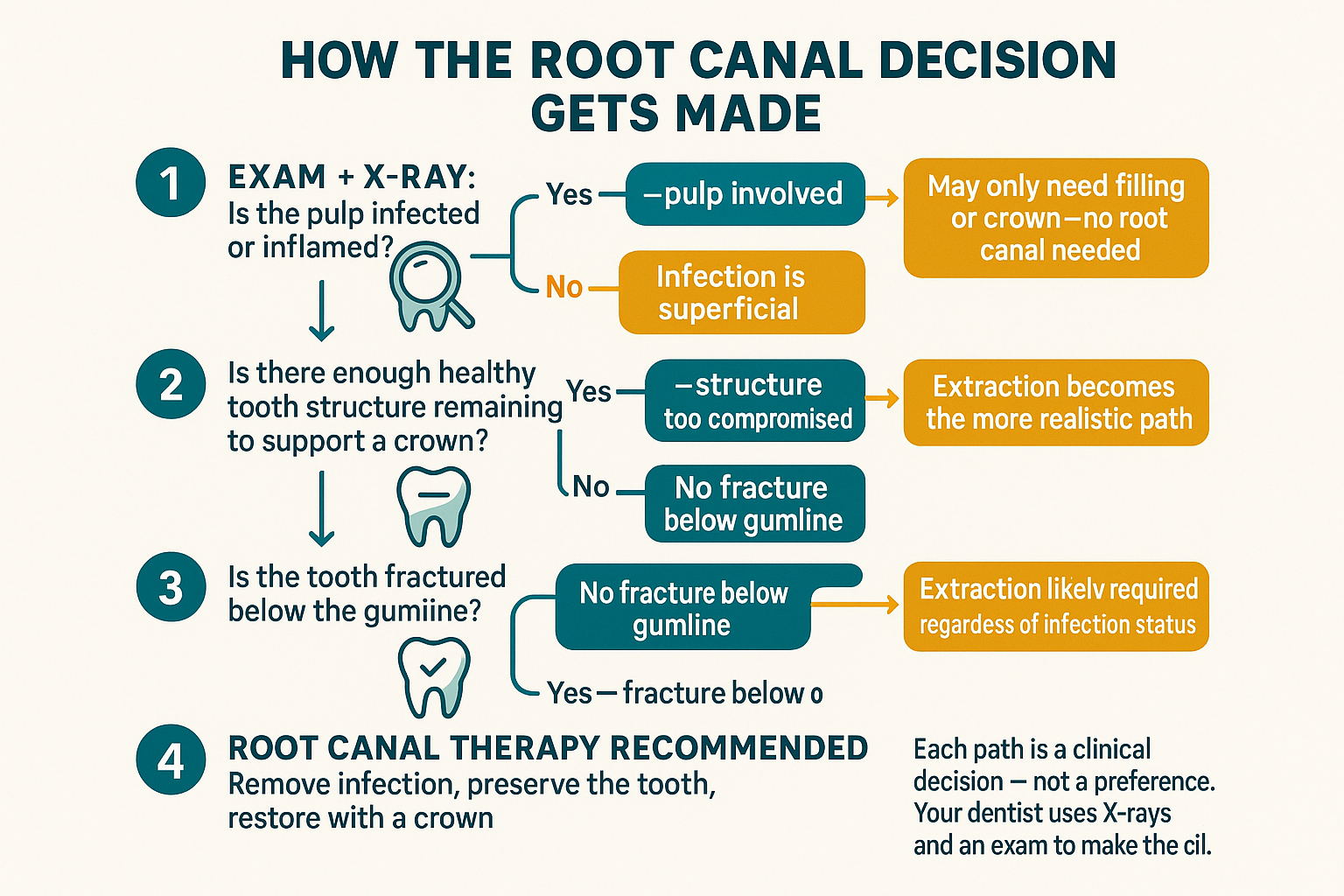
How the Root Canal Decision Gets Made: A Clinical Path
This diagram shows the decision points a dentist moves through when evaluating a painful or infected tooth — from initial exam to treatment recommendation.
What the In-Office Experience Actually Looks Like
A lot of patients who’ve been putting off care have a specific fear in their head — usually built on a story they heard years ago, or a procedure they had as a kid. The actual experience of modern endodontic treatment is usually very different from that mental picture.
One patient described her experience this way: “She is very clear and gentle. My broken tooth was fixed painlessly and I was able to be seen right away.” — Xiang N.
That word — clear — comes up often. Patients who’ve avoided the dentist because they didn’t know what to expect tend to feel more at ease once someone walks them through what’s actually going to happen, step by step, before anything begins.
Root canal therapy is performed under local anesthetic. For most patients, the procedure itself is not painful — the discomfort people associate with it is often the infection that preceded it. Some tenderness in the 1–3 days after treatment is normal as the tissue heals. Most patients return to normal activity the next day.
For patients with significant dental anxiety, there are comfort-focused options worth discussing during your consultation. How to Tell If a Dental Practice Is Actually Built for Anxious Patients is a useful read if that’s part of what’s kept you from calling.
What It Means to Have an In-House Endodontist
For patients in Renton and the surrounding South King County area, one of the more practical differences at Cedar Dental Group is that Dr. Joe Dutner — our in-house endodontist — is here at 280 Hardie Ave. SW. That means if your tooth needs root canal therapy, you don’t get referred out to a separate specialist’s office, wait for an opening in their schedule, drive somewhere new, and then come back to us for the crown.
The whole sequence — diagnosis, endodontic treatment, and restorative follow-up with a crown — happens in one place. For patients who’ve already felt overwhelmed by fragmented care, or who delayed treatment partly because the logistics felt like too much to manage, that continuity matters.
It also means the endodontist and the restorative dentist are working from the same records, the same X-rays, and the same treatment plan. Nothing gets lost between offices. The crown that gets placed afterward is planned from the start with the full picture in mind — not added on at a different practice months later.
If it turns out extraction and an implant are the right path instead, Dr. Kim — our board-certified periodontist — handles the surgical side of that process in-house as well. You’re not starting over with a new provider at each stage.
Frequently Asked Questions About Root Canal Therapy and Alternatives
Is there really an alternative to root canal therapy that saves the tooth?
Not in most cases where the pulp is infected. Some patients ask about antibiotics as an alternative — antibiotics can reduce swelling and temporarily quiet symptoms, but they don’t clear the infection from inside the tooth. The infection returns. Root canal therapy is the only treatment that actually removes the source of infection while keeping the tooth. If a tooth is genuinely unsalvageable, extraction followed by an implant or bridge is the realistic alternative — but that’s replacing the tooth, not saving it.
How do I know if my tooth actually needs a root canal or if it’s something less serious?
You can’t tell from symptoms alone, and neither can we without an exam. Persistent throbbing pain, sensitivity to heat, pain when biting, or swelling near the tooth are all signs the pulp may be involved — but a dental X-ray is what actually shows whether the infection has reached the root. Some teeth with pulp infection have very little pain. The only way to know is to get it evaluated.
What happens if I just pull the tooth instead of doing a root canal?
Extraction is a legitimate option in the right clinical situation, and it’s sometimes the correct call. But if the tooth could have been saved, extraction starts a longer process: you lose the tooth, the bone underneath it begins to resorb over time, and replacing it with an implant takes 3–6 months or more, at significantly higher cost than a root canal and crown. A bridge is a faster option but requires shaping the adjacent healthy teeth. Neither outcome is bad — they’re just more involved than preserving the original tooth when that’s still possible.
Does a root canal hurt?
The procedure itself is performed under local anesthetic, and most patients report that the tooth pain before treatment was worse than the treatment itself. Some soreness in the 1–3 days after is normal. Modern endodontic techniques have changed significantly from what most people picture when they hear ‘root canal.’
My tooth has been hurting for about two weeks. Is it too late for a root canal?
Not necessarily — but the longer an infection goes untreated, the more the tooth structure and surrounding bone can be affected. A tooth that was a strong candidate for root canal therapy two weeks ago may or may not still be at the same stage now. The only way to know is an exam. If you’ve had ongoing pain, it’s worth calling sooner rather than continuing to wait.
Do I need a referral to see an endodontist for a root canal?
At Cedar Dental Group, no. Dr. Dutner is our in-house endodontist, so if root canal therapy is the right treatment for your tooth, there’s no referral process or separate specialist to track down. Dr. Chu handles the evaluation and restorative work; Dr. Dutner handles the endodontic procedure — all at the same office on Hardie Ave. in Renton.
Ready to Get a Straight Answer About Your Tooth?
If you’ve been sitting on tooth pain and trying to figure out what you’re actually dealing with, an exam is the only way to get a real answer. Cedar Dental Group sees patients from Renton, Tukwila, Kent, Newcastle, and across South King County — and with Dr. Dutner on-site, you won’t be sent somewhere else if root canal therapy turns out to be the right path. Call us at 425-430-0400 or visit cedardentalgroup.com to schedule a consultation.