
Direct Answer: A crown restores a tooth that still has its root. A bridge replaces a missing tooth using neighboring teeth as anchors. An implant replaces the root and tooth entirely, without touching adjacent teeth.
We see it often in our form submissions — someone writes in saying they have a broken tooth and need an implant or a veneer, and they’ve already made up their mind before they’ve talked to anyone. That’s not a criticism. It means they’ve been doing research, which is exactly the kind of patient I enjoy working with. But the decision they’ve landed on doesn’t always match what their actual situation calls for.
Crowns, bridges, and implants are not interchangeable. Each one addresses a different clinical problem, involves a different timeline, and carries different long-term trade-offs. Choosing the wrong one — or skipping the diagnostic step that would tell you which one fits — can mean spending more money later to correct something that wasn’t set up right.
This article walks through how that decision actually gets made, what the real differences are between these three options, and how your insurance timing can affect which path makes the most sense this year versus next.
The Core Distinction: What Each Option Actually Does
Before comparing costs or timelines, it helps to be clear on what problem each restoration solves.
A crown is a cap that fits over a tooth that still has a viable root. The tooth itself is damaged — cracked, decayed, or worn down — but the root is healthy enough to support a restoration. The crown protects what’s left and restores full function. Think of it as rebuilding the visible part of a tooth that’s still anchored in place.
A bridge is used when a tooth is already gone. It spans the gap by anchoring artificial tooth to the two teeth on either side of the space. Those neighboring teeth have to be permanently reshaped — filed down — so the bridge can bond to them. It’s a reliable restoration that’s been used for decades, but it does permanently alter otherwise healthy teeth to make room.
An implant also replaces a missing tooth, but it does something the bridge doesn’t: it replaces the root. A titanium post is placed into the jawbone, a healing period follows, and then a crown is attached on top. The adjacent teeth are never touched. And because there’s an artificial root in the bone, you avoid the bone loss that happens over time when a tooth is missing.
These three options solve three distinct problems. The one that’s right for you depends on whether your tooth is still there, what condition the surrounding teeth are in, and how much bone volume you have if the tooth is already gone. For a deeper look at the implant decision specifically, When Is a Dental Implant the Right Choice After Tooth Loss? walks through that question with more detail.
Why Crown Material Matters More Than Most Patients Realize
One of the questions that comes up less than it should is: what is the crown actually made of? Most patients focus on whether they need a crown at all. But the material affects durability, appearance, how the crown interacts with neighboring teeth, and how long it’s likely to last.
The two most common options right now are zirconia and porcelain-fused-to-metal (PFM).
Zirconia crowns are milled from a single solid material — no metal core underneath. They’re strong, they don’t show a dark line at the gumline as the gum recedes over time, and they tend to look more natural. They’re also gentler on opposing teeth than older ceramic materials.
Porcelain-fused-to-metal crowns have a metal interior with a porcelain layer on the outside. They’ve been around for decades and are well-understood. But the metal core can show over time, especially near the gum. And the porcelain layer can be harder on the tooth it bites against.
For front teeth, appearance usually drives the material conversation. For molars that take significant chewing force, strength and fit are the priority. Dr. Chu walks through material choices with each patient as part of the crown planning process — because which material is right depends on where the tooth is, what your bite looks like, and what your long-term goals are. If you want to go deeper on what separates a well-fitted crown from a poor one, What Makes a Crown Actually Fit Well? is worth reading before your consultation.
The Crown After a Root Canal Question
One of the most common moments of surprise I see is when a patient comes in for a root canal and learns they’ll also need a crown on the same tooth. It feels like two procedures instead of one, and the cost adds up fast.
But there’s a straightforward reason for it. During root canal therapy, the pulp — the nerve and tissue inside the tooth — is removed and the canals are sealed. That process requires access through the tooth, which means removing a significant amount of tooth structure. What’s left is more brittle than a living tooth and much more prone to fracture under normal chewing forces.
A crown placed over a root-canal-treated tooth protects it from cracking. For back teeth especially — molars and premolars that absorb most of your chewing load — skipping the crown after a root canal puts the tooth at high risk of fracturing in a way that can’t be repaired. At that point, the tooth is lost anyway, and you’re back to bridge versus implant.
So the two procedures aren’t separate recommendations stacked on top of each other. They’re part of the same treatment plan to actually save the tooth long-term.
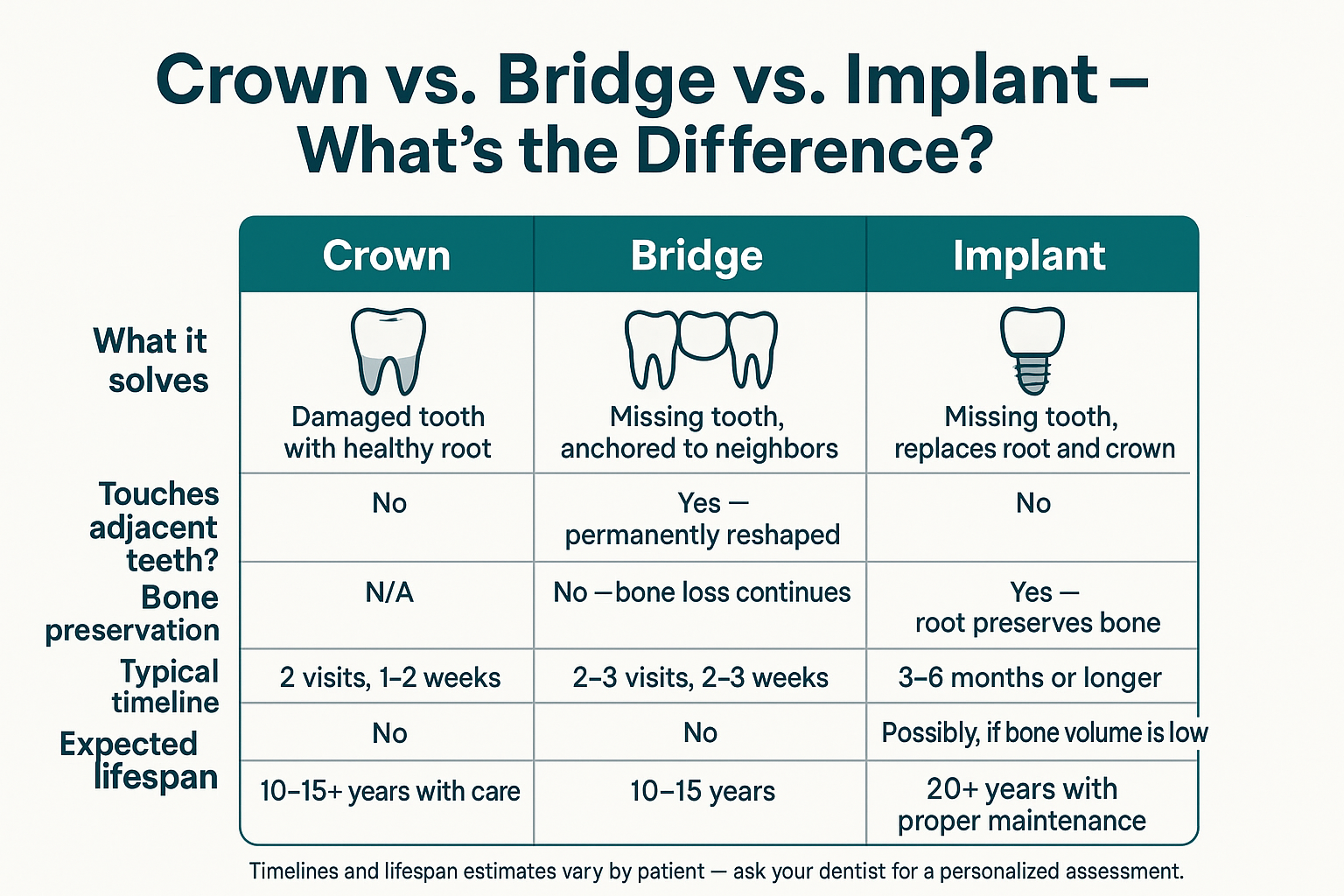
Crown vs. Bridge vs. Implant: Side-by-Side
This comparison lays out the three restorations across the factors that matter most when making a treatment decision.
How Insurance Timing Affects the Decision
A lot of patients right now are activating new dental coverage — we’ve seen several form submissions recently from people who just got insurance through work and are ready to finally address things they’ve been putting off. Here’s why benefit year timing matters when you’re looking at a multi-step restoration.
| Restoration Type | Typically Insurance-Covered? | Timing Consideration |
|---|---|---|
| Crown | Yes, partially — usually 50% after deductible | Can often be completed within one benefit year |
| Bridge | Yes, partially — usually 50% after deductible | Can often be completed within one benefit year |
| Implant (post + crown) | Varies widely — post often not covered; crown sometimes is | Multi-stage process may span two benefit years — plan accordingly |
| Bone graft (if needed before implant) | Rarely covered; some plans include partial coverage | Often completed same year as implant post placement |
Why Insurance Timing Can Actually Shape Your Treatment Plan
Most dental plans have an annual maximum — a cap on what they’ll pay out in a given benefit year, commonly somewhere in the range of $1,000 to $2,000, though this varies by plan. Once you hit that number, any remaining costs are out of pocket until the new year resets your benefits.
For a crown or bridge, you can usually start and finish within a single benefit year. That makes it easier to predict what you’ll spend and what insurance will cover.
Implants are different. The process typically involves multiple stages spread over months — consultation and imaging, any bone grafting if needed (which I’d encourage you to read about at Why Bone Grafting Comes Up — and What It Actually Means for Your Timeline), placement of the implant post, a healing period, and then the final crown. Intentionally planning the early stages in one benefit year and the crown placement in the next can let you apply two years of insurance maximums toward the same case.
This is worth discussing at your consultation — not as a hard rule, but as something to factor in when you’re weighing options and timelines. Our front desk team can also help verify your specific plan’s coverage before you commit to a treatment direction.
When the Answer Isn’t Obvious — What Actually Happens at the Appointment
A lot of patients come in having already decided what they need. Sometimes they’re right. But the clinical picture doesn’t always match what someone researched online.
For example: someone with a broken tooth might assume implant is the only real option. But if the root is still intact and healthy, a crown may restore full function without any surgical procedure. Or a patient who comes in expecting a simple crown might have bone loss that changes the picture entirely once we take imaging.
The evaluation step — X-rays, clinical exam, and a conversation about your goals — is what actually determines which option fits. At Cedar Dental Group, Dr. Chu handles that initial assessment and walks through the findings with you before any recommendation is made. If the situation involves bone loss or gum-related factors, Dr. Kim’s periodontal expertise is available in-house, which means you’re not waiting on a referral to get a complete picture.
For anyone weighing the implant path specifically, How Long Does the Dental Implant Process Actually Take? gives a realistic look at the full timeline from evaluation to final crown.
Frequently Asked Questions About Crowns, Bridges, and Implants
My tooth is broken but it doesn’t hurt. Do I still need a crown?
Pain isn’t always a reliable signal of how serious a crack or break is. A broken tooth that feels fine now can fracture further under chewing pressure, which can turn a straightforward crown into a tooth extraction. An X-ray and clinical exam will show whether the root and surrounding bone are healthy — that’s the real indicator, not how it feels day to day.
Can I get a bridge instead of an implant to save money?
A bridge is generally less expensive upfront than an implant, and for many patients it’s a solid long-term option. The trade-off is that the two teeth on either side of the gap have to be permanently filed down to anchor the bridge — even if those teeth are otherwise healthy. Over time, the bone under the missing tooth also continues to shrink since there’s no root stimulating it. An implant preserves that bone. Neither is automatically the right choice — it depends on your bone volume, the condition of adjacent teeth, and your long-term goals.
Why do I need a crown after a root canal? Can’t I just leave it?
After a root canal, the tooth loses the internal moisture and flexibility that a living tooth has. It becomes brittle and much more likely to crack under normal chewing forces — especially on back teeth. A crown protects the tooth from fracturing. Skipping it on a molar is a common way to end up losing a tooth that could have been saved for years longer.
How do I know if I have enough bone for an implant?
That’s determined through imaging — typically a 3D cone beam scan — that shows the height and width of bone at the implant site. If bone volume is low, a bone graft may be recommended first to create a stable foundation. This is a separate procedure from the implant itself, with its own healing timeline.
Does dental insurance cover implants?
Coverage varies widely by plan. Some plans cover the implant crown (the visible tooth portion) but not the implant post itself. Others exclude implants entirely. A few plans have begun covering a portion of the post. The only way to know for sure is to have your specific plan verified — which our team can do before you schedule anything. It’s also worth asking whether phasing treatment across two benefit years could help you apply more coverage to the total cost.
What’s the difference between zirconia and porcelain-fused-to-metal crowns?
Zirconia is a single solid material — strong, natural-looking, and it doesn’t develop a dark line at the gumline over time. Porcelain-fused-to-metal (PFM) has a metal core with porcelain on the outside. PFM has a long track record, but the metal can show near the gum as you age, and the porcelain can be harder on opposing teeth. For most patients today, zirconia is the more common recommendation — but placement location and your bite pattern factor in too.
Ready to Get a Clear Answer for Your Specific Situation?
If you’ve been going back and forth on crowns, bridges, or implants — or you’ve already decided but want to make sure the decision actually fits your situation — the right next step is a consultation where we can look at real imaging and talk through your goals. We’re located in Renton and serve patients across South King County, including Tukwila, Kent, Burien, and Newcastle. You can reach us at 425-430-0400 or visit cedardentalgroup.com to schedule a time that works for you.