
Direct Answer: You likely need a gum graft when the root surface is exposed, sensitivity is measurable, or recession is actively progressing. A periodontist evaluation is the only way to know for certain.
You noticed something. Maybe a cold drink hit sharper than it used to. Maybe you looked in the mirror and one of your teeth looked a little longer. Maybe your dentist mentioned a gum graft at your last visit and you left with more questions than answers. That kind of observation sends a lot of people searching for “how do I know if I need a gum graft”, and I want to give you a real answer, not a vague one.
Gum recession is not a single condition with a single response. It exists on a spectrum, and where you fall on that spectrum determines everything, whether you monitor and wait, whether you change your brushing habits, or whether a graft becomes a genuine clinical recommendation.
What I can do here is walk you through how to read your own symptoms, what the evaluation actually looks for, and how the decision gets made. By the end, you’ll have a much clearer sense of where you likely stand.
What Your Symptoms Are Actually Telling You
Cold sensitivity is the symptom that sends the most people searching. And there’s a straightforward reason it happens.
When gum tissue recedes, the root surface of the tooth becomes exposed. That root surface is made of cementum, which is porous and doesn’t have the same protective enamel layer that covers the rest of the tooth. When cold water or air hits cementum, the sensation travels to the nerve faster and sharper than you’d feel on the crown of the tooth. That’s not in your head, it’s a structural reality.
A tooth that looks longer than it used to is another clear signal. Teeth don’t actually grow longer as adults. What you’re seeing is the gumline pulling back, exposing more of the tooth’s surface. If the change is visible to you in a mirror, there’s measurable recession happening.
Other things worth paying attention to:
- A toothbrush stroke at the gumline that feels distinctly tender or sharp
- A gumline that looks uneven between neighboring teeth
- A notch or groove at the base of a tooth near the gum margin
- Any area where the gum looks thin, pale, or like it’s pulling away
None of these symptoms automatically mean you need a graft. But they do mean the tissue deserves a closer look, and that closer look is what separates monitoring from action.
Gum Recession Is a Spectrum, Here’s How to Think About Where You Fall
This is probably the most important thing I can tell you: the question isn’t whether you have recession. It’s how much, how stable, and how much tissue is left.
Mild recession, a millimeter or two, with a healthy band of firm attached gum tissue still present, is often managed through better brushing technique, softer bristles, and more frequent periodontal maintenance visits. The American Academy of Periodontology recognizes that early-stage recession can often be stabilized without surgery when the contributing factors are addressed and the tissue that remains is thick and healthy.
More significant recession changes the math. When the root surface is visibly exposed, when the band of attached gum tissue is thin or nearly gone, or when recession appears to be progressing between visits, a graft becomes a genuine conversation. Attached tissue is important because it acts as a physical barrier that resists further pulling. Once that tissue is thin or absent, the recession tends to continue.
Active progression is the key variable. Stable recession that has been the same for years is a very different situation than recession that has measurably worsened since your last exam. A periodontist can take precise measurements at each visit to track whether the recession is holding steady or moving, and that data drives the recommendation more than the absolute millimeter count alone.
For more on how gum disease and recession relate to each other and what separates a deep cleaning from a surgical conversation, Gum Surgery vs. Deep Cleaning: How Patients Know Which One They Need goes into that distinction in detail.
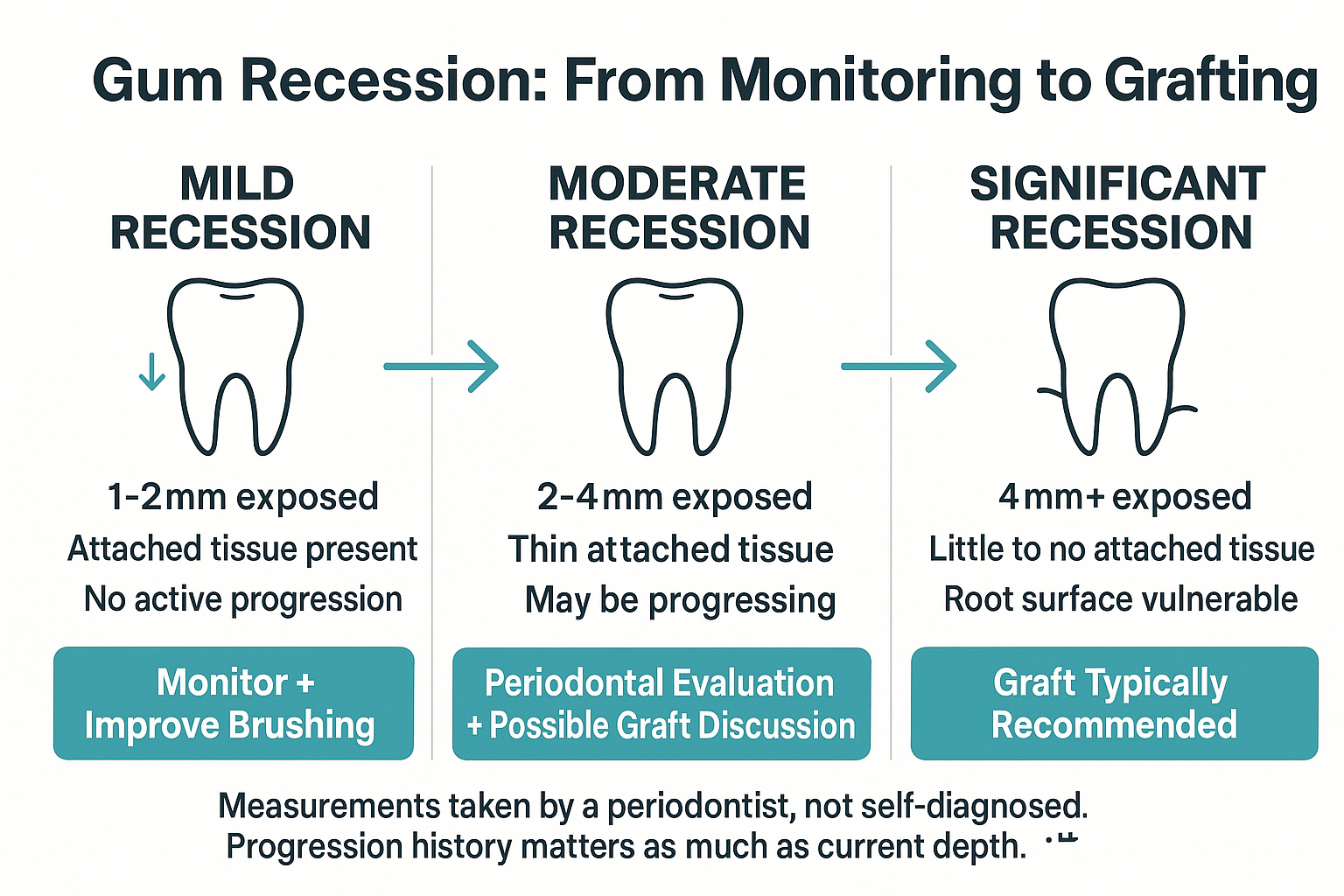
The Gum Recession Severity Spectrum
This overview shows how recession severity maps to typical clinical responses, from monitoring to grafting.
Is a Gum Graft Cosmetic or Medically Necessary? The Answer Affects Your Insurance
This is a question I hear often, and it’s worth being direct about: a gum graft can be either, or both, depending on your specific situation.
When recession is exposing the root in a way that creates measurable sensitivity, puts the tooth at risk of structural damage, or is creating conditions that could lead to bone loss, that typically falls into medically necessary territory. Insurance coverage is more predictable in those cases, though it’s never guaranteed without verification.
When the recession is primarily aesthetic, the gumline looks uneven, a tooth appears longer than its neighbors, but the tissue is stable and no root damage is occurring, coverage becomes less predictable. Some plans cover a portion even in those cases; others don’t. The distinction matters because it affects how patients think about timing and out-of-pocket cost.
What I’d suggest before you call anyone about insurance: get a clear diagnosis first. Knowing the clinical reason behind the recommendation, whether it’s protecting a vulnerable root, stopping active progression, or improving gumline symmetry, helps you have a much more productive conversation with your insurance provider. A well-documented clinical chart note from a board-certified periodontist carries weight in that process.
For a broader look at what goes into surgical costs when bone is also involved, Why Bone Grafting Comes Up, and What It Actually Means for Your Timeline is worth reading, since recession and bone loss sometimes travel together.
Graft vs. Monitor: What Typically Drives the Recommendation
This table summarizes the clinical factors that generally push a case toward monitoring versus grafting, though only a direct evaluation can determine what applies to your situation.
| Clinical Factor | Suggests Monitoring | Suggests Graft Evaluation |
|---|---|---|
| Amount of recession | 1-2mm, stable | 3mm or more, or actively progressing |
| Attached gum tissue | Healthy band present | Thin, minimal, or absent |
| Root surface exposure | Minimal, covered by tissue | Visible root surface on exam |
| Cold sensitivity | Mild or absent | Sharp, consistent, or worsening |
| Recession trend | Stable for 1+ years | Measurably worse since last exam |
| Risk of bone loss | Low risk currently | Root exposed near bone crest |
What Happens If You Wait, Without the Alarm
This is the question a lot of people carry into their research and don’t always get a straight answer on. So I’ll give you one.
Gum tissue does not grow back on its own. Once the recession has occurred, that tissue stays gone unless it’s surgically replaced. That’s not said to frighten anyone, it’s just the biology. A graft works by taking tissue (often from the roof of the mouth, or from processed donor tissue) and placing it over the exposed root area, where it integrates and builds back the gumline.
What matters most when deciding whether to wait is whether the recession is stable or moving. Stable recession that isn’t progressing, isn’t causing significant sensitivity, and still has healthy attached tissue present is a reasonable case for monitoring. Waiting doesn’t necessarily make things worse if the underlying causes, aggressive brushing, grinding, untreated gum disease, have been addressed.
Recession that is progressing is a different situation. Each millimeter of tissue lost makes a future graft more complex, because there’s less surrounding tissue for the graft to attach to. Waiting in a progressing case doesn’t buy time; it narrows options.
A periodontist can measure pocket depths, track recession severity over time, and assess the amount of remaining attached tissue to tell you clearly which category you’re in. That clinical picture, not a symptom list or a mirror, is what determines whether monitoring is safe or whether waiting is adding complexity to a future procedure. You can read more about what the recovery side of grafting looks like in Gum Grafting Recovery: What the First Two Weeks Actually Look Like.
What the Evaluation Actually Looks Like, and Who Does It
At Cedar Dental Group, gum grafting and periodontal evaluations are handled by Dr. Jaewon Kim, a board-certified periodontist who sees patients in-house. That means if you’re already a patient here or come in for a new-patient exam and recession is identified, you don’t get handed a referral slip to schedule a separate appointment at a different office weeks from now.
Dr. Kim takes precise measurements of recession depth at each affected site, evaluates the width and thickness of remaining attached gum tissue, and assesses whether active progression is occurring. That data shapes the recommendation, and it gives patients a clear, documented picture of where they stand rather than a vague impression.
For patients in Renton and the surrounding South King County area who’ve been putting off this evaluation because the referral process felt like too many steps, having this level of specialist care available in one location makes the process simpler. The evaluation itself is not complicated or uncomfortable, it’s a clinical measurement visit, and most patients find it far less involved than they expected.
If you’re also wondering about gum disease treatment that may have happened before a graft conversation came up, Deep Cleaning Helped, So Why Is Surgery Still Being Recommended? addresses exactly that situation and is worth a read before your visit.
Frequently Asked Questions About Gum Grafts
My dentist mentioned a gum graft but didn’t say it was urgent. Should I be worried?
Not necessarily. A mention at a routine visit often means your dentist noticed recession worth tracking, not that something is about to go wrong. The follow-up question to ask is whether the recession is stable or progressing, and whether you have a healthy band of attached tissue still present. Those two factors shape everything. If your dentist flagged it, ask them to point you toward a periodontist for a measurement-based evaluation so you have a real answer to work with.
Can changing my brushing technique prevent recession from getting worse?
Yes, in some cases. Aggressive brushing is one of the most common contributors to recession, particularly on the outer surfaces of lower front teeth and upper back teeth. Switching to a soft-bristle brush and using a lighter, circular motion rather than a horizontal scrub can stop brushing-related recession from progressing. But if the recession is caused by gum disease, grinding, or thin tissue from birth, brushing changes alone won’t be enough. A periodontist can tell you which factor is driving yours.
How much does a gum graft typically cost?
Cost varies significantly based on how many teeth are involved, the type of graft used, and what your insurance covers. When the procedure is documented as medically necessary, exposed root, measurable sensitivity, active progression, insurance often covers a portion, though out-of-pocket costs still vary by plan. For a more predictable estimate, an in-person evaluation is the right starting point. We can review your coverage and walk through what to expect before you commit to anything.
Will a gum graft fix my cold sensitivity?
For most patients, yes. When sensitivity is caused by an exposed root surface, grafting tissue back over that root often reduces or fully resolves the sensation. The cementum that was exposed to temperature and touch gets covered again, and the sensitivity fades as the tissue heals. Results vary by individual, but sensitivity reduction is one of the most consistently reported outcomes after grafting.
Is there a difference between a gum graft and gum surgery?
Yes, and it matters. A gum graft is a specific procedure that adds tissue to an area of recession, covering an exposed root and rebuilding the gumline. Periodontal surgery refers to a different category of procedures, like flap surgery or regenerative surgery, which address advanced gum disease by accessing the structures below the gumline. They’re distinct procedures treating distinct conditions. If your provider recommended one or the other, it’s worth asking them to explain specifically what they’re addressing and why, the reasoning should be clear.
I’ve had recession for years and it hasn’t changed. Do I still need to get it evaluated?
Long-standing stable recession is generally lower risk than recession that’s actively moving. But ‘it hasn’t changed’ is hard to confirm without measurements taken at regular intervals. If you haven’t had a periodontal evaluation that includes documented recession depths, you may not have a real baseline to compare against. Getting measured now gives you an actual reference point, and if things really are stable, that’s a reassuring answer to have in writing.
Ready to Get a Clear Answer on Where You Stand?
If you’ve been sitting with a graft recommendation, a sensitivity you can’t explain, or a gumline that just doesn’t look right, the most useful thing you can do is get a measurement-based evaluation from someone who specializes in exactly this. We see patients from Renton, Kent, Tukwila, Newcastle, and across South King County who come in with exactly these questions and leave with a real picture of their situation. To schedule a periodontal evaluation with Dr. Kim or to ask questions before you commit, call us at 425-430-0400 or visit cedardentalgroup.com to learn more.