

Direct Answer: Gum recession gets worse gradually. The warning signs are tooth sensitivity, teeth that look longer, and discomfort near the gumline. Catching it early gives you more options.
A lot of people in Renton first notice something is off not from pain, but from a tooth that looks a little longer than it used to. Or maybe brushing near the gumline suddenly feels sharp. You’re not imagining it — these are real early signs that your gum tissue is receding, and they’re worth paying attention to before things progress.
The tricky part about gum recession is that it moves slowly. Most people don’t notice it until it’s already been happening for months or years. By then, the root surface of the tooth may be exposed, which opens the door to sensitivity, decay on the root, and eventual bone loss if nothing changes.
This post is for patients who are in the discovery phase — noticing something but not sure yet if it’s serious. We’ll walk through what mild recession looks like versus progressing recession, and what actually makes a difference in stopping it.
The Signs That Tell You Recession Is Moving in the Wrong Direction
Gum recession isn’t something you wake up with overnight. It tends to creep, which means the window to catch it early is longer — but it also means patients often wait too long without realizing it.
Here are the signals that most commonly bring patients in:
- A tooth that looks visibly longer than the teeth around it
- Sensitivity to cold, heat, or brushing along the gumline — not from cavities, but from exposed root surface
- A notch or divot you can feel with your tongue at the base of a tooth
- Gums that look darker pink or slightly translucent near the margin
- Discomfort that wasn’t there six months ago when your hygienist cleaned that area
Any one of these on its own isn’t necessarily an emergency. But two or more together, especially with sensitivity that’s new or worsening, is a signal worth getting checked.
The distinction that matters most isn’t whether you have recession — it’s whether it’s stable or actively progressing. Stable recession in one or two spots can sometimes be managed with changes to brushing habits and more attentive hygiene. Progressing recession, especially when it’s exposing root structure, is a different clinical situation entirely. That’s the line where doing nothing starts to cost you more than acting.

Mild Recession vs. Progressing Recession: What’s the Actual Difference?
Not all gum recession is treated the same way, and not all of it requires surgery. Understanding the difference helps you know what questions to ask at your next visit.
Mild recession usually means the gumline has pulled back slightly — often 1 to 2 millimeters — but the tissue is still attached, there’s no significant root exposure, and sensitivity is minimal or occasional. In these cases, the main goals are stopping the cause and monitoring closely.
Changes that can slow or stabilize mild recession:
- Switching to a soft-bristled toothbrush and brushing with lighter pressure
- Correcting brushing technique — scrubbing side to side accelerates recession significantly
- Getting a night guard if clenching or grinding is contributing
- Treating underlying gum disease with a deep cleaning (scaling and root planing) if inflammation is present
Progressing recession is a different situation. This is when the tissue continues to pull back despite good hygiene, when the root is now exposed and collecting plaque and tartar more easily, or when sensitivity has moved from occasional to consistent. At this stage, the tissue loss is unlikely to stop on its own.
This is also when a procedure like gum grafting enters the conversation — not as a cosmetic choice, but as a way to protect the tooth long-term. If you’re wondering whether your situation has crossed that line, this guide on knowing when recession is serious enough to need a graft goes deeper on that specific decision.
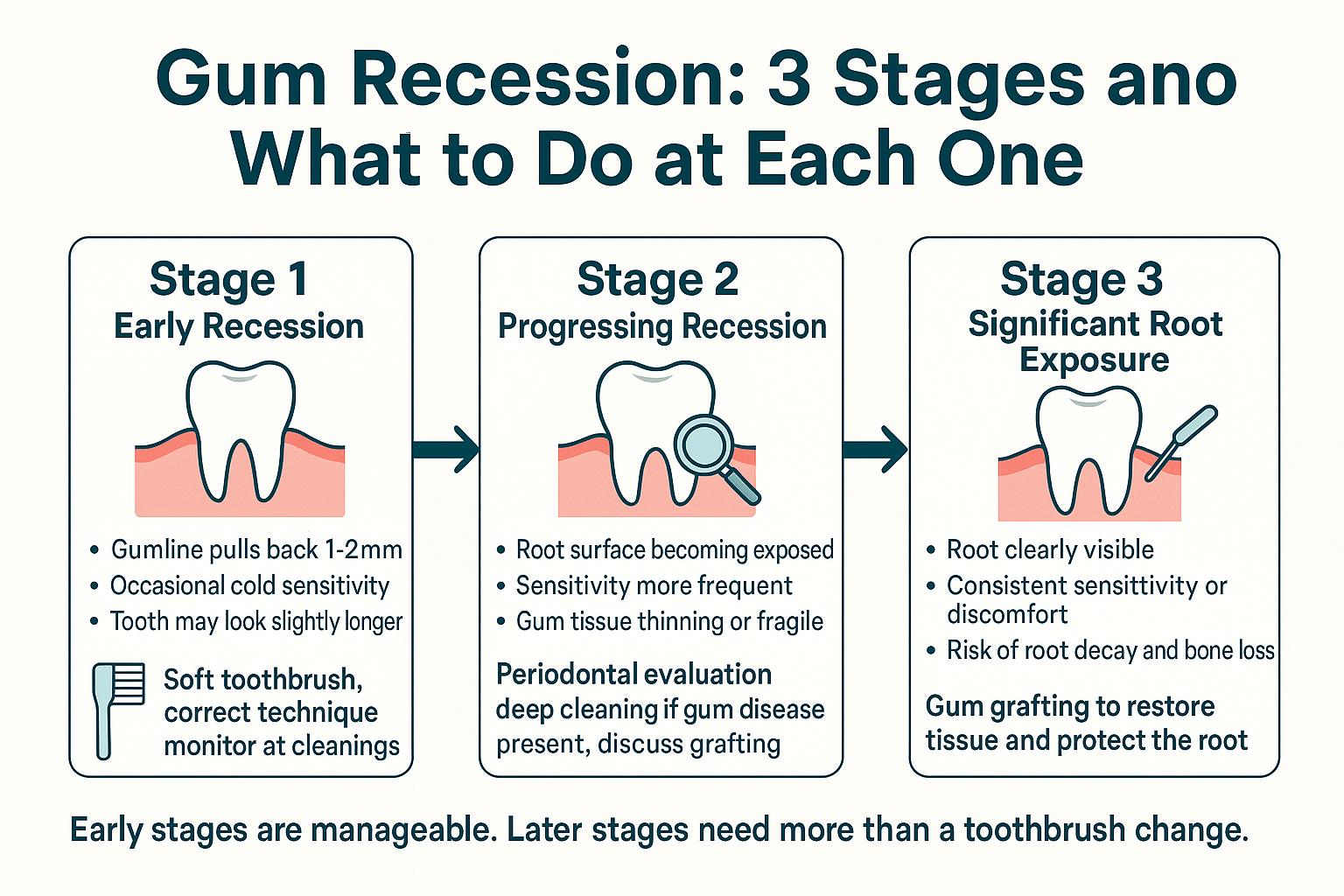
The Recession Progression: From Early Signs to When Action Matters
This infographic shows the three stages of gum recession — what each looks like clinically, what the patient typically feels, and what the recommended response is at each point.
What Gum Grafting Actually Involves — and What Recovery Looks Like Honestly
If your recession has progressed to the point where grafting is recommended, here’s what the procedure actually involves so you’re not going in blind.
A connective tissue graft — the most common type — takes a small amount of tissue from the roof of your mouth (the donor site) and attaches it to the area where gum tissue has been lost. This restores the protective coverage over the root and helps rebuild a stable gumline.
At Cedar Dental Group, grafting is performed by Dr. Jaewon Kim, a board-certified periodontist. That matters practically because most general dental offices refer patients out to a separate specialist — often a 2 to 6 week wait just to get a consultation, then another wait for the procedure itself, with two different offices managing your care. Having Dr. Kim in-house means those steps happen in one place, with one coordinated treatment relationship from evaluation through recovery.
For a deeper look at what the procedure itself involves, this patient guide to gum grafting surgery covers the clinical steps in plain language.
On recovery — here’s what to actually expect:
The first 3 to 5 days are the most uncomfortable, and most of that discomfort comes from the donor site on the roof of the mouth, not the graft site itself. Patients typically describe it as feeling like you burned the roof of your mouth on hot pizza — tender, but manageable.
During that window:
- You’ll be on a soft diet — think yogurt, scrambled eggs, mashed potatoes, smoothies
- Talking a lot is uncomfortable, so patients who can protect some quiet recovery time do better
- Over-the-counter pain medication handles most of the discomfort for most patients
- By day 7 to 10, most people are back to a fairly normal routine
One practical note: summer scheduling has a real advantage here. If you have flexibility in July or August, recovery is easier to protect when your schedule is naturally lighter — fewer back-to-back work commitments, more ability to rest and eat soft food without it being a disruption.
If dental anxiety is part of what’s been keeping you from addressing this, this guide to finding a dental practice built for anxious patients may be a useful read before your consultation.
Recession Stage at a Glance: What’s Typical and What It Usually Means
This table gives a quick reference for understanding where your situation likely falls and what kind of response each stage typically calls for.
| Recession Stage | What You Might Notice | Typical Next Step |
|---|---|---|
| Early / Stable | Slightly longer-looking tooth, rare sensitivity | Adjust brushing habits, monitor at cleanings |
| Progressing | More frequent sensitivity, thin or fragile gumline | Periodontal evaluation, possible deep cleaning |
| Root Exposed | Visible root surface, consistent sensitivity or discomfort | Gum grafting evaluation with a periodontist |
| Root Exposed + Bone Loss | Mobility, significant sensitivity, bone showing on X-ray | Periodontal surgery or bone grafting may be needed |
What Actually Stops Recession From Getting Worse
There’s no toothpaste that reverses recession — lost gum tissue doesn’t grow back on its own. But recession that’s caught early can often be stabilized, which means it stops progressing even if it doesn’t fully reverse.
The most effective things that actually stop recession from worsening:
1. Fix the mechanical cause first.
If aggressive brushing is the driver — and it often is — no procedure will hold long-term unless the technique changes. A soft brush, light pressure, and small circular motions protect tissue better than the scrubbing motion most people use.
2. Treat active gum disease.
Recession caused by advanced gum disease won’t stabilize while infection is still present. Scaling and root planing (a deep cleaning) is often the first step before any surgical consideration.
3. Address grinding or clenching.
Patients who grind at night put significant lateral force on teeth, which accelerates gum and bone loss over time. A well-fitted night guard is one of the less glamorous but genuinely useful interventions.
4. Get grafting done before bone is involved.
This is the part most patients don’t realize: gum recession left long enough eventually affects the underlying bone. Once bone loss enters the picture, the treatment becomes more involved — and more expensive. Grafting earlier, when it’s a gum tissue issue only, is a much simpler procedure than treating recession that has already reached the bone level.
Frequently Asked Questions About Gum Recession
Can receding gums grow back on their own?
No. Once gum tissue is lost, the body doesn’t regenerate it. The goal of early intervention is to stop the recession from continuing — not to reverse what’s already happened. Grafting can restore coverage over exposed roots, but it’s a surgical solution, not a natural one.
My tooth is sensitive to cold but I don’t see anything wrong. Could it still be recession?
Yes, absolutely. Cold sensitivity near the gumline is one of the most common early signs of root exposure, and it often shows up before recession is visually obvious. If sensitivity is new or getting worse, it’s worth having it looked at — even if nothing looks dramatically different to you in the mirror.
How do I know if I need a gum graft or just better brushing habits?
That’s exactly the right question to ask, and it’s one that requires a clinical look — not a self-diagnosis. In general: if recession is mild, stable, and not causing consistent sensitivity or root exposure, better technique may be enough to stop it. If it’s progressing, if the root is visible, or if sensitivity is getting worse, grafting is usually the recommendation. This guide on knowing when recession needs a graft can help you think through it before your appointment.
Is gum grafting painful?
The procedure itself is done under local anesthesia, so you shouldn’t feel pain during it. Recovery is the more relevant concern — the donor site on the roof of the mouth is typically the main source of discomfort for the first 3 to 5 days. Most patients manage it with over-the-counter pain medication and a soft diet. By the end of the first week, most people are doing well.
Does dental insurance usually cover gum grafting?
When grafting is done for medical or functional reasons — to protect a root, stop progression, or prevent bone loss — most dental insurance plans cover a portion of it, typically treating it as a periodontal procedure rather than cosmetic. Coverage varies by plan, so it’s worth a benefits check before your consultation.
Why does it matter that the periodontist is in-house vs. a referral?
Practically speaking, it means no waiting weeks for a separate specialist appointment, no repeating your health history to a new office, and no gap between whoever diagnosed the problem and whoever treats it. Dr. Kim works alongside Dr. Chu, so your care is coordinated from the start. For patients who already feel some anxiety about dental treatment, having that continuity in one familiar place makes a real difference.
Ready to Get a Clear Answer on Where Your Gums Actually Stand?
If something feels off — a tooth that looks longer, sensitivity that’s new, or a gumline that doesn’t look even — the most useful thing you can do is get a real look at it. Cedar Dental Group serves patients throughout Renton and the surrounding South King County area, including Kent, Tukwila, and Newcastle. You can call us at 425-430-0400 or visit cedardentalgroup.com to schedule a consultation with Dr. Kim or Dr. Chu and find out exactly what your situation calls for.